
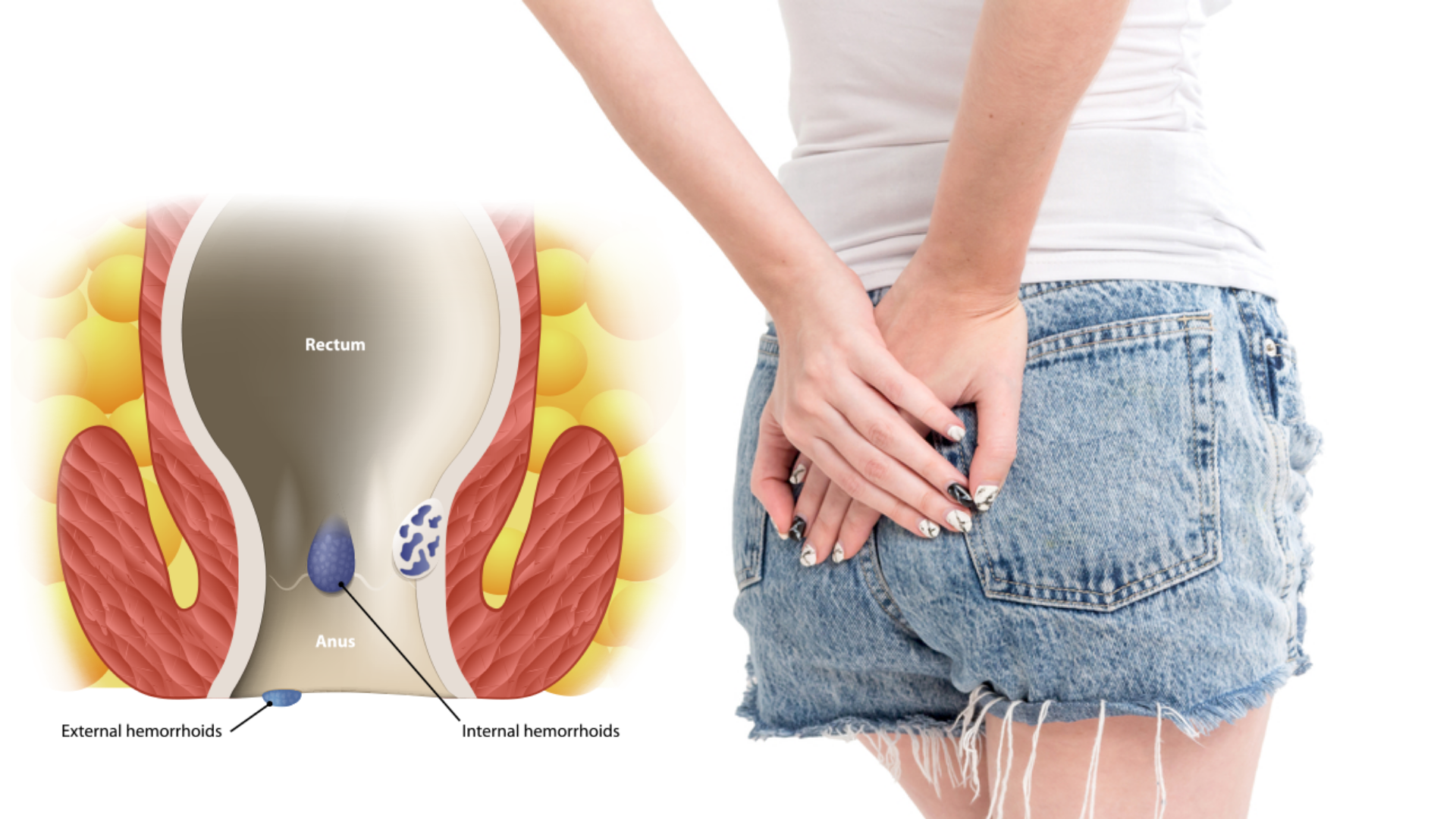
Hemorrhoids rubber band ligation is a very common treatment to painlessly eliminate hemorrhoids in an outpatient clinic. This modality of treatment is generally called instrumental treatment of hemorrhoids.
To understand what the indications for instrumental treatment are, one must have in mind the classification of hemorrhoids.
GRADES are a simple (though not the only) conventional system of classifying hemorrhoids:
• 1st degree: small hemorrhoids, which never prolapse (come out);
• 2nd degree: haemorrhoids that prolapse, but which spontaneously shrink;
• 3rd degree: haemorrhoids that prolapse and that the patient must manually reduce (which do not fall on their own)
• 4th degree: hemorrhoids that can no longer be reduced.

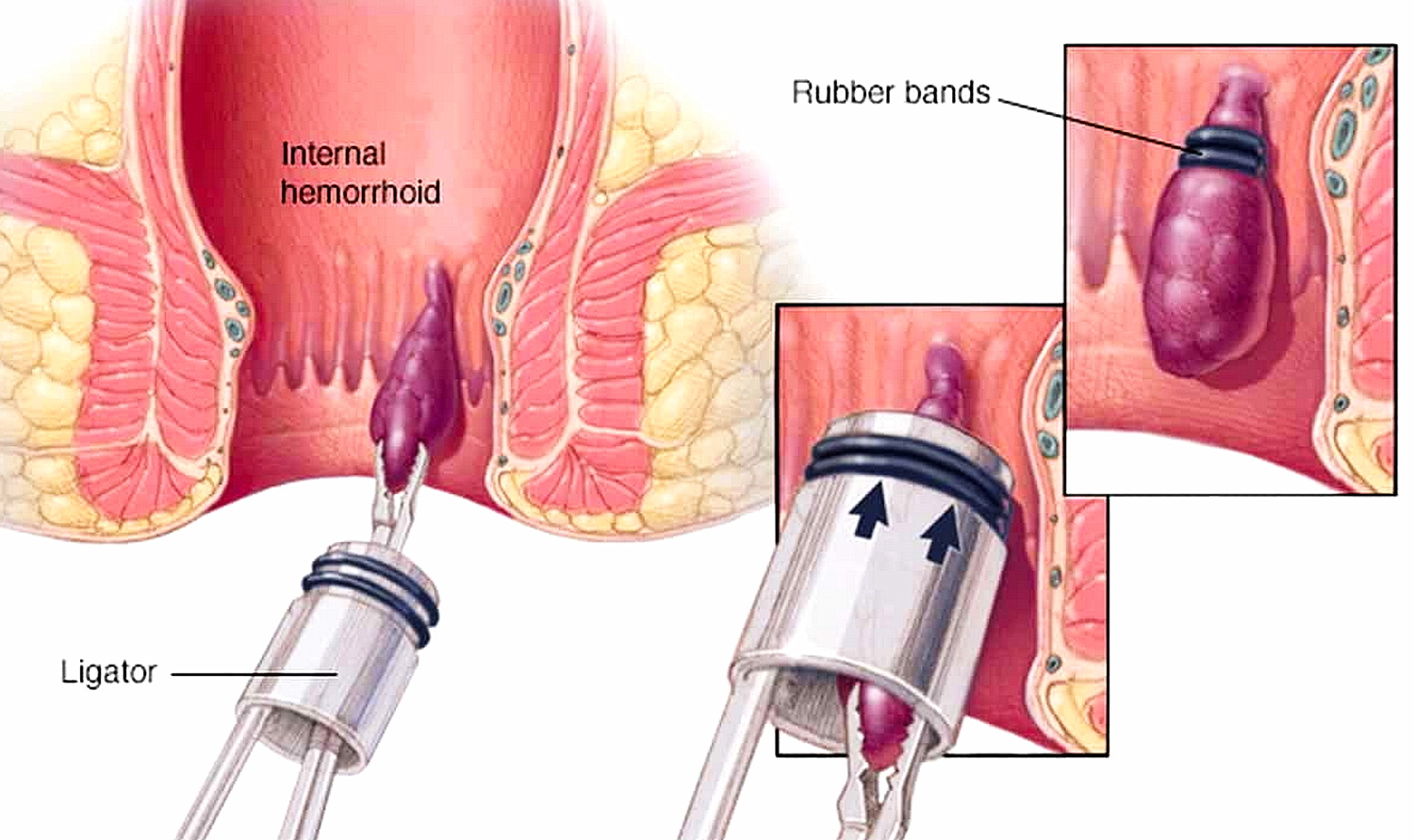
Hemorrhoids rubber band ligation, what it consists on?
The traditional indications for Hemorrhoids rubber band ligation treatment concern the I and II degree; in reality, outpatient practice has shown that not infrequently even grade III hemorrhoids can be cured, thus avoiding surgery.
The elastic ligation consists in placing an elastic at the base of the haemorrhoidal gavocciolo: in practice, with a special “gun” the haemorrhoidal tissue is lifted, aspirating it into a cylindrical cannula, and a small elastic is “fired”. With sclerosis, a drug, kinurea, is injected into the subhemorrhoidal mucous tissue and into the hemorrhoid itself, which acts by inducing an inflammatory reaction which, on the one hand, occludes the hemorrhoidal vascular complex, and on the other “fixes” the hemorrhoidal cushions to the most superficial layers of the rectal wall.
The protocol we have standardized for many years includes 6 sessions of ligations, spaced 15 days apart, followed by two sclerosis sessions with kinurea, also 15 days apart.
The security of this protocol is very high. Although in the literature it is reported that even three hemorrhoidal pads could be tied at a time, in reality what is obtained with the ligation is ischemia and the subsequent fall of the tied area, with the formation of a scar that fixes the mucous membrane of the rectum to the underlying muscle planes.
Increasing the ischemic area, by tying more than one hemorrhoidal gallop at a time, increases the risk of perforation of the rectal wall (an extremely serious event, which causes an infection of the perirectal soft tissues which, in the most unfortunate cases, can lead to the patient’s death ), and therefore the most prudent course of action is to limit the ligature to one hemorrhoid at a time. As further evidence, we happened to visit patients with severe hemorrhoidal prolapses and urgent surgical indication, caused by ligation of three or more hemorrhoids at once.
The Hemorrhoids rubber band ligation, when well done, is very fast and practically painless: the patient may feel a kind of discomfort, as a stimulus to defecation without being able to do it, in the first hours after ligation, and little more. This discomfort depends on the size of the tethered gavocciolo and can be treated simply by taking metamizole, paracetamol, or any other analgesic half an hour before the session.
A few days after the ligation, the strangled gavocciolo detaches and is eliminated with the faeces, generally without the patient noticing anything: at most, the presence of a little blood on the toilet paper is noticed, always depending on the dimensions of the tied buoy.
Pain is practically absent, since the tied area is devoid of sensory innervation: the treatment does not need any type of anesthesia and does not in any way limit the normal daily activities of those who undergo it.


